Cancer in the Time of COVID-19 in Japan: Collateral Damage
Pandemic-induced panic had alarming effects on cancer diagnosis and treatment in Japan.

The people of Japan watched with the rest of the world as the saga of the Diamond Princess Cruise Ship unfolded and hospitals in Wuhan, China filled up with COVID-19 patients early last year. In response, the people of Japan, along with the Japanese government, media, medical establishment, panicked.
Japan declared a state of emergency three times over the course of the pandemic (7 April, 8 July 2020, and 25 April 2021). However, despite the repeated state of emergency declarations, Japan did not and has not adopted the strict lockdown measures observed in the US and some European countries. The Japanese government instead asked its citizens to restrict their activities voluntarily.
This voluntary approach to the pandemic has yielded apparently good COVID outcomes. As of 17 May 2021, with a population of 126 million, Japan has had 685,135 COVID cases and 11,471 COVID deaths. Compared to the US (330 million population, 32,940,841 cases, and 585,970 deaths) or the UK (68 million population, 4,466,589 cases, and 127,941 deaths), the impact of COVID in Japan has been much more limited.i
However, the panic about COVID in Japan has caused some collateral harm. Caring for cancer patients and screening the population to catch cancer in its early stages were laid aside when the government recommended that people delay physical exams, including screening tests. Fearing COVID outbreaks, many hospitals terminated routine treatments, shut down operating rooms, and cancelled surgical procedures to biopsy or remove cancer. Japanese cancer patients responded by avoiding hospitals because they feared COVID more than cancer.
Though the panic has subsided to some degree, the damage in the form of worse cancer outcomes will continue to accrue. Many Japanese hospitals, which stayed empty just in case COVID cases were to rise, remain empty – especially smaller hospitals with fewer than 200 beds. This article provides a short description of COVID and its impact on cancer care in Japan.
The Collapse of Inpatient Care in Japan
As a health economist, I have been tracking the workings of Japanese hospitals and clinics for 30 years. Through the Japanese health policy think tank that I run, Global Health Consulting Japan (GHC), I have compiled data from 454 large acute care hospitals, representing a significant fraction of all inpatient care in Japan.ii Over the course of the epidemic, these hospitals have treated 28,247 COVID patients, accounting for approximately 30% of inpatient COVID inpatient cases in Japan.iii
Image 1, immediately below, shows changes (year-by-year in the same month) in the number of scheduled hospital admissions between March and December 2020 for the top 20 most frequent diagnostic categories in these hospitals.
* * *

* * *
The impact of COVID on the Japanese medical system was swift and dramatic. During the first wave, scheduled hospital admissions in diagnostic categories such as cataract, angina, nonmalignant disorders of the small intestine, and inguinal hernia dropped sharply in March 2020 and were cut in half by May. This is because both physicians and patients decided to postpone non-essential elected surgeries and procedures during the pandemic. Cancer care, however, continued.
Readers should note that though cataract and inguinal hernia surgeries, cardiac catheterizations, and polypectomies are performed primarily in outpatient settings in the US and elsewhere, they are typically performed during hospital admissions in Japan. Japan has the highest number of acute care beds per 1,000 inhabitants among OECD countries.iv Japanese hospitals have strong supply-side incentives to keep their beds occupied. Japanese hospitals’ average length of stay is also the longest among OECD countries.v
After dramatic initial drops in care for many patients (including cancer patients) during the first two epidemic waves, things appeared to return to somewhat normal in October 2020–and then the third COVID-19 wave hit Japan.
Missed Detection, Delayed Diagnoses and Treatments
As we have seen, cancer screening and surgery were sharply disrupted in Japan. Unlike many non-cancer services like cataract operations that declined immediately after the start of the epidemic in March, the sharp drop in cancer care started later, with the peak decline in July and August 2020 rather than in May. There is a straightforward explanation for this delayed impact on cancer.
Commonly, cancers in Japan are detected either at routine visits at primary physicians/small local hospitals or at complete annual physical examinations required to be provided to all workers by their employer according to Japanese law.vi After detection, patients are referred to regional cancer centres to confirm clinical diagnoses and for necessary treatments.
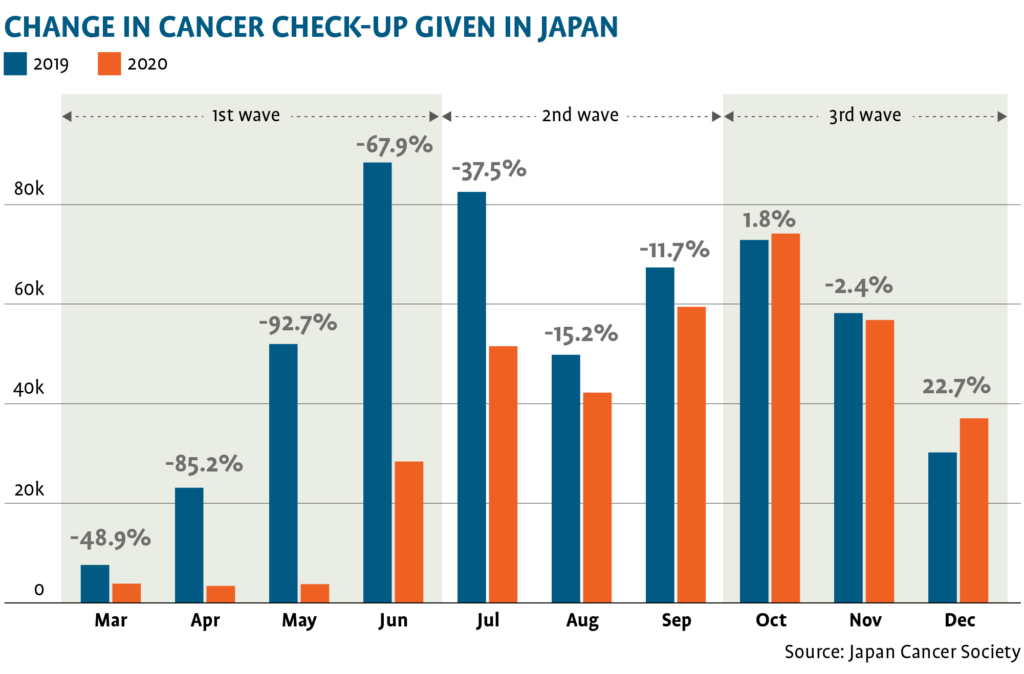
Referrals of suspected cancer patients from primary physicians/small local hospitals to regional cancer centres were effectively halted during the COVID pandemic. Following the state of emergency on 7 April 2020, the Japan Society of Health Evaluation and Promotion (JSHEP) announced a recommendation to delay non-essential physical examination and screening. According to a survey by the Japan Cancer Society (JCS), cancer screenings (stomach cancer, lung cancer, colon cancer, breast cancer, and uterine cancer) declined more than 90% in May 2020 compared with May 2019 (Table 2). The JSC estimated that at least 10,000 cancer cases went undetected in Japan due to the halt in physical examinations and cancer screenings.
* * *
* * *
It typically takes 2 to 3 months between the initial detection of cancer and a patient receiving treatment (e.g., surgery, chemotherapy, or radiotherapy). Routine cancer screening and medical examinations continued in March and April 2020 so that there were still enough accumulated cancer patients (scheduled appointments) for regional cancer centres to stay busy until the early summer.vii The delayed and dramatic decline of scheduled cancer patients in July and August is due to the stoppage of cancer screening and medical examinations after April.
Implications
Even though Japan has relied upon self-quarantine rather than a strict lockdown like England or the US, the COVID-19 pandemic has caused significant disruption in cancer diagnosis and management. What are the possible implications of these delays?
One careful meta-analysis for seven cancers (bladder, breast, colon, rectum, lung, cervix, and head and neck) concluded that cancer patients whose treatment is delayed by even one month have a 6 to 13% higher risk of dying.viii Another study estimated the impact of diagnostic delays of 12 months and found substantial increases in the number of avoidable 5-year cancer deaths in England.ix Yet another study of the collateral damage from the lockdowns found that a 3-month delay in surgery for cancer patients in England led to more than 4,700 additional deaths in England.x
The panic caused by the pandemic has had alarming effects on cancer diagnosis and treatment. Deaths from COVID have fortunately been limited so far in Japan. Ironically, perhaps, Japan may end up suffering greater “collateral damage” from saving COVID patients – in the form of sharply higher cancer deaths – than from COVID itself.
* * *
References
i Johns Hopkins Coronavirus Resource Center, https://coronavirus.jhu.edu/
ii Our COVID study database contains anonymous patient and encounter-level information collected over the 24-month period between January 1, 2019, and December 31, 2020. The data were originally collected from hospital forms that were submitted to the Japanese government as part of an ongoing effort to reform the healthcare reimbursement system in Japan. Hospitals that participate in this program are designated as Diagnosis Procedure Combination (DPC) hospitals, and together, they account for more than half of all the acute care beds in Japan. The DPC hospitals represent approximately 20% of all hospitals in Japan; they include all major academic medical centers and most of the nation’s larger hospitals. Our sample encompasses 100% of the patients from roughly half of these DPC hospitals. The data contain information on patient status at admission and discharge; cost of admission; and details on surgeries, procedures, and drugs administered during the patient’s stay at the hospital. In total, our data encompass information for approximately 3.8 million patients in more than 450 hospitals located across every region of Japan.
iii Between March 1 and December 31, 2020, there were 233,773 PCR positive cases and an estimated 83,015 COVID inpatient admissions in Japan.
iv OECD, https://www.oecd.org/coronavirus/en/data-insights/hospital-beds-acute-care
v OECD, https://data.oecd.org/healthcare/length-of-hospital-stay.htm
vi Under Japan’s universal health insurance system, every Japanese citizen can receive medical services with modest copayments and all the employers are required to provide their workers medical examinations by a physician annually by the Industrial Safety and Health Act (Article 66).
vii Japan Society of Medical Oncology (JSMO) announced that surgeries for early-stage cancers can be delayed up to four weeks or switched to chemotherapy or radiotherapy depending on patient conditions. JSMO stated that those who were receiving postoperative adjuvant chemotherapy should continue as planned but frequency of chemotherapy cycle can be changed e.g., once every other week to once every three weeks. For those not yet started on postoperative adjuvant chemotherapy, JSMO stated that adjuvant chemotherapy could be delayed depending upon risk of recurrence, overall condition, underlying diseases, side effects, etc.
viii Timothy Hanna et al. “Mortality due to cancer treatment delay: systematic review and meta-analysis” BMJ 2020;371:m4087.
ix Camille Maringe et al., “The impact of the COVID-19 pandemic on cancer deaths due to delays in diagnosis in England, UK: a national, population-based, modelling study” Lancet Oncol 2020; 21(8):1023-1034.
Dr. Aki Yoshikawa, a health economist, is a founder and chairman of Global Health Consulting Japan (GHC). GHC is the pioneer of the health care benchmarking analysis in Japan. Prior to GHC, Dr. Yoshikawa was the Associate Director of the Comparative Health Care Policy Research Project at Stanford University.
x Amit Sud et al. “Collateral damage: the impact on outcomes from cancer surgery of the COVID-19 pandemic” Annals of Oncology 2020 Aug; 31(8):1065-1074.